
Defensive Inference and Systemic Risk in Korean Biopharma
When Statistical Weakness Becomes a Due Diligence Threat
Complete text: 백신을 위한 변호 — 안전성과 효과에 대한 우려의 최신 근거
- 요즘 백신에 대한 불안을 호소하시는 분들의 이야기를 많이 듣습니다. 지인의 이상반응을 가까이서 본 분, 또 막연한 불안 속에서 뉴스를 따라가시는 분들까지 그 감정은 모두 이해가 갑니다. 저 또한 연구자이기 이전에 같은 감정을 가진 사람이기 때문입니다.
- 한국은 팬데믹 이전까지 백신 신뢰도가 세계 최고 수준이었습니다. 그런데 지금은 전 세계에서 가장 큰 폭으로 신뢰도가 하락한 나라가 되었습니다. 그 사이에 무엇이 있었는지를, 과학자로서 정리해볼 필요가 있다고 생각합니다.
- 백신 데이터를 많이 다루어 본 전문가로서 제가 드릴 수 있는 것은, 지금까지 축적된 가장 충실한 근거를 있는 그대로 보여드리는 일이라고 생각합니다. 감정이 아니라 숫자와 데이터로 말입니다.
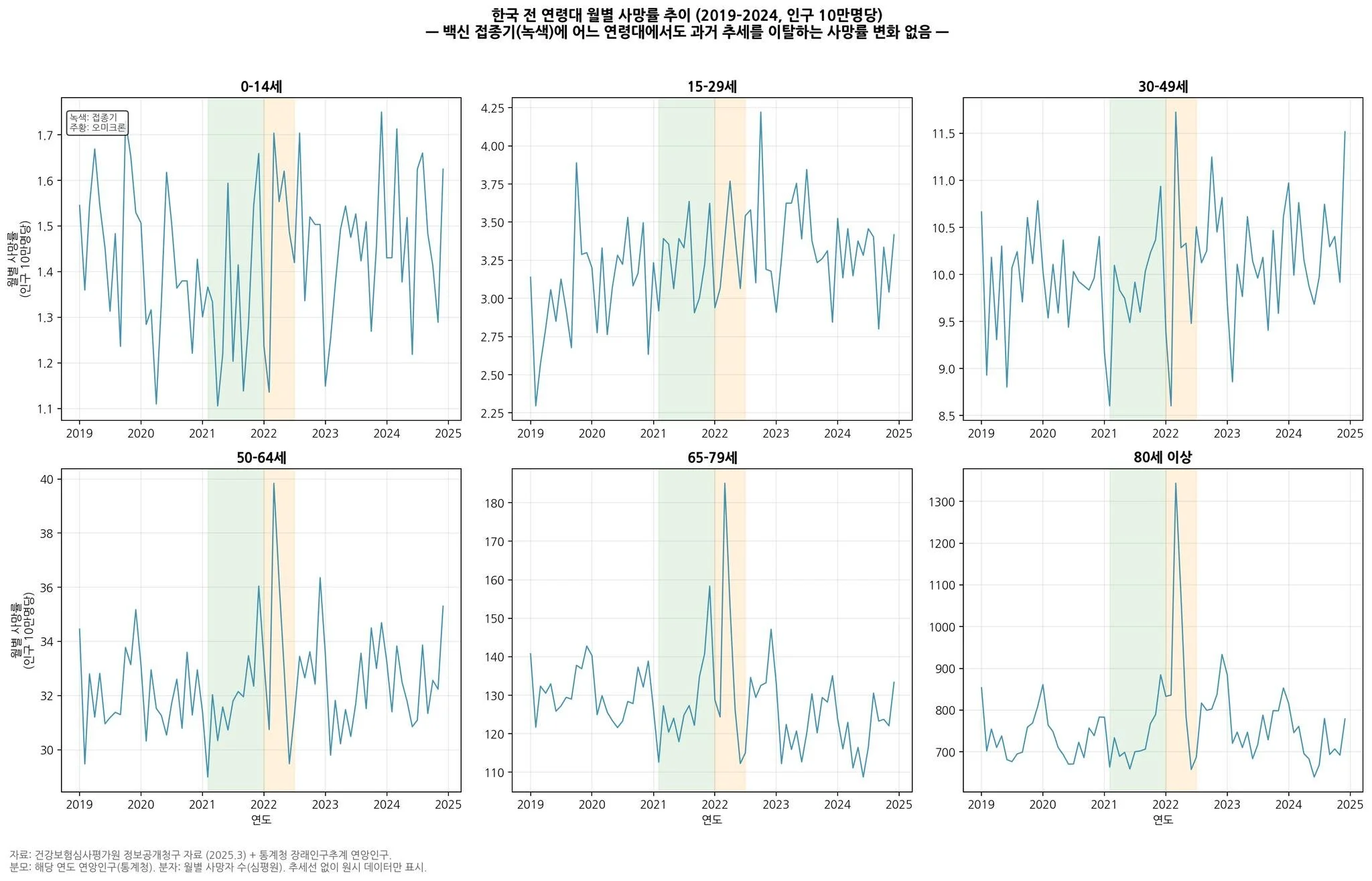
1. 접종이 가장 많이 이루어진 시기에, 한국의 초과사망은 오히려 가장 적었습니다 — 연령별 사망도 마찬가지입니다
- 2021년은 전 국민이 사실상 처음으로 대규모 mRNA·아데노바이러스 백신을 맞은 시기입니다. 만약 백신이 전체 사망을 증가시키는 방향으로 작용했다면, 이 시기에 초과사망(예년 추세 대비 늘어난 사망)이 가파르게 올라가야 했습니다.
- 그러나 대한민국은 2021년 접종 시작 직후 6개월의 초과사망이 거의 0에 가깝거나 음수였던 나라입니다. 초과사망이 본격적으로 증가한 시점은 2021년 11-12월 델타변이 바이러스 유행과 2022년 2-4월 오미크론 대유행기였고, 이는 접종 시작 시점과 시간적으로 분리됩니다
- 그렇다면 혹시 특정 연령대에서만 사망이 늘었는데 전체 통계에 묻힌 것은 아닐까요? 이 질문에 답하기 위해 저희 연구팀은 건강보험심사평가원 정보공개청구 원시자료를 직접 분석했습니다.
- 결과는 명확합니다. 초기 접종이 활발하게 이루어졌던 시점에서 어느 연령대에서도 접종 시기에 과거 추세를 이탈하는 사망 증가가 관찰되지 않았습니다. 0–14세, 15–29세, 30–49세, 50–64세, 65–79세, 80세 이상 — 모든 연령군에서 2021년 접종 시기의 사망률은 예측치와 달라지지 않습니다. 사망이 뚜렷하게 증가한 시점은 2022년 상반기 오미크론 유행기였고, 이는 접종이 아니라 감염 자체의 영향입니다. 월별 데이터로 해상도를 더 높여봐도 같은 결과입니다.
- 접종이 사망률을 높였다면 나올 수 없는 그림입니다. 전체로 봐도, 연령대별로 쪼개 봐도, 월별로 확대해 봐도 마찬가지입니다. 이것이 한국 데이터의 가장 중요한 근거입니다. 첫 번째 그림입니다.
2. 암 발생률도 과거의 추세를 이탈하지 않았습니다
- "백신이 암을 일으킨다"는 이야기는 여러 해 반복되어 왔습니다. 최근 Biomarker Research (2025)에 실린 한국 서울 지역 대규모 코호트 연구가 SNS에서 많이 인용되는데, 이 연구의 오류는 이미 제가 여러 번 지적을 했습니다.
- 더 중요한 것은, 우리나라 인구집단의 코호트별 암발생률이 2015–2023년 사이 큰 추세 변화를 보이지 않는다는 점입니다. 2020년의 일시적 감소는 팬데믹 초기 건강검진 지연이 만든 진단 지연 효과이며, 2021년 반등은 검진이 정상화되며 쌓였던 진단이 한꺼번에 잡힌 결과입니다. 전 국민의 80% 이상이 접종을 받은 2022–2023년에도 암 발생률의 비정상적 급증은 관찰되지 않았습니다.
- 이 질문에 더 엄밀하게 답하기 위해, 저희 연구팀은 국민건강보험공단(NHIS) 자격·청구 데이터를 질병관리청 예방접종등록 자료와 연계하여 전국민 규모의 중단시계열분석을 수행했습니다.
- 결과는 12개 암종(구강·인두, 소화기계, 호흡기·흉곽내, 뼈·관절연골, 흑색종·피부, 중피종·연조직, 유방, 여성생식기, 남성생식기, 비뇨기계, 눈·뇌·중추신경, 림프·조혈계) 모두에서 관찰된 월별 발생률이 반사실적 예측의 99% 예측구간 안에 위치했으며, 수준 변화와 추세 변화 모두 통계적으로 유의하지 않았습니다. 출생 코호트별 하위분석과 개입 시점 변동 민감도 분석에서도 결과는 일관되었습니다.
- 쉽게 말하면, 백신 접종이 본격화된 이후에도 한국인의 암 발생률은 접종 전 추세에서 벗어나지 않았고, 이는 12가지 암 모두에서 동일한 결론입니다. 두 번째 그림입니다.
3. 드물지만 치명적인 이상반응은 존재합니다. 그리고 우리는 그 데이터를 감추지 않고 공개합니다.
- 백신은 완벽한 의약품이 아닙니다. 대중이 100% 안전한 의약품을 기대하는 것은 자연스럽지만, 현실에서 모든 의료 행위에는 기회비용이 존재합니다. mRNA 백신의 심근염, 아데노바이러스 벡터 백신의 혈전성 혈소판감소 증후군(TTS) 같은 이상반응은 실제로 존재하고, 극히 드물지만 치명적일 수 있습니다. 저를 비롯한 연구자들은 이 이상반응들을 국내 데이터로 분석해 국제학술지에 보고해왔습니다.
- 다만 편익과 피해의 비대칭성을 말씀드려야 합니다. 백신 접종으로 인한 집단적 편익(사망 및 중증화 예방)은 부작용으로 인한 위험보다 매우 큽니다.
- Watson 등이 Lancet Infectious Diseases (2022)에 발표한 연구는, 코로나19 백신으로 접종 첫 해에만 전 세계적으로 약 1,980만 명의 사망이 예방되었다고 추정했습니다. 백신이 없었다면 3,140만 명이 사망했을 것이라는 반사실적 시나리오 대비, 접종을 통해 63%의 사망을 막은 셈입니다.
- 질병관리청(KDCA)과 국내 연구진의 분석에 따르면, 22년까지 60세 이상 고령자에서 백신의 중증 감염 예방 효과는 91.6%, 사망 예방 효과는 92.3%였습니다 (Kim et al., Osong Public Health and Research Perspectives 2023). 예방된 중증 사례의 83.5%, 예방된 사망의 93.0%가 60세 이상 고령자에서 발생하여, 백신이 가장 취약한 집단을 가장 많이 보호했음을 보여줍니다.또 국내에서만 접종을 통해 112,195명의 사망을 막아낸 것으로 평가됩니다.
- 이상반응의 절대 위험도를 비교하면 그 편익의 규모가 더 선명해집니다. 영국 3,800만 접종자 대상 자기대조 환자군 연구(Patone M et al., Nature Medicine 2022)에서는 mRNA 백신 접종 후 심근염 추가 발생은 접종 100만 명당 약 1-6건이었고 SARS-CoV-2 감염 후에는 100만 명당 약 40건의 추가 심근염이 발생하여, 백신보다 감염 자체가 심근염 위험을 6~40배 더 높였습니다.
'저희의 의무는 이 데이터를 가감 없이 공개하는 것입니다. 그것이 과학이 신뢰를 얻는 유일한 방법이기 때문입니다.'
- 그리고 동시에 말씀드려야 할 사실이 있습니다. 코로나19 백신은 이제 역사상 가장 많은 안전성 데이터가 축적된 백신입니다. "개발 기간이 짧아 안전성 데이터가 부족하다"는 주장은 대표적인 오해입니다. 통상 10년이 걸리는 백신 개발 기간은 기술적 한계 때문이 아니라, 백신 자체의 낮은 시장성(수익성)으로 인한 자금 조달과 임상 참여자 모집의 지연 때문입니다. 팬데믹 상황에서는 전 세계적 위기감 속에서 천문학적인 공공 펀딩과 국가 주도 지원이 이루어졌기에 개발 기간을 획기적으로 단축할 수 있었습니다. 오히려 코로나19 백신은 가장 짧은 기간 내에 가장 방대한 규모의 안전성 데이터가 임상과 실제 처방 환경 양쪽에서 검증된 의약품입니다.
- 전 세계 수십억 회분의 접종에 대해 사전·사후 능동감시(V-safe, KAERS, VAERS, EudraVigilance, 영국 Yellow Card 등)가 이루어졌고, 한국에서도 수백만 명 단위의 국가 데이터베이스 기반 인과성 분석이 수십차례 발표되었습니다. 데이터가 없어서가 아니라, 데이터가 많기 때문에 우리가 드물지만 실재하는 위험까지 이야기할 수 있는 것입니다.
5. 그렇다면 우리는 왜 백신을 의심하게 되었을까요
- 여기서부터는 과학보다는, 인간의 마음에 대한 이야기입니다.
첫째, 통계와 경험의 간극, 그리고 보상의 부족입니다. 인구 전체를 놓고 보면 백신의 편익은 압도적이지만, 바로 옆 가족이 이상반응을 겪은 분에게 확률이 낮다는 말은 결코 위로가 되지 않습니다. 특히 우리나라는 코로나19 이전에는 백신 이상반응에 대한 감시체계나 평가 기전, 데이터베이스가 매우 부족했습니다. 코로나19 이후 많은 개선이 있었지만, 이상반응 피해자에 대한 제도적 인정과 보상이 충분히 따뜻하지 못했다는 점은 저도 많이 아쉽게 생각합니다. 조금 더 미리 잘 준비가 되었다면 하는 아쉬움이 큽니다. 이러한 불안은 보상 제도의 강화와 안전성에 대한 지속적 소통을 통해 계속 보완해나가야 합니다.
둘째, 불확실성에 대한 과도한 단순화와 방역 과정에서의 압력입니다. 과학은 본디 "모른다"와 "현재까지의 최선의 추정" 사이에서 움직입니다. 그러나 언론소통 과정 등에서 이 미묘함이 종종 완전한 안전과 효과라는 단정으로 번역되었고, 예외 사례가 발견될 때마다 신뢰가 한꺼번에 무너지는 일이 반복되었습니다. 또한 팬데믹이라는 위기 상황에서 접종이 개인의 자율적 선택이라기보다 방역패스, 시설이용 제한 등 사회적 압력의 형태로 유도된 측면이 있었습니다. 공중보건의 관점에서 신속한 접종률 달성이 절실했던 것은 사실이지만, 그 과정에서 개인의 자기결정권이 충분히 존중받지 못했다는 인식은 결국 백신뿐 아니라 방역 정책 전반에 대한 의구심으로 연결되었습니다. 돌이켜보면 '왜 맞아야 하는지'에 대한 설명보다 '맞지 않으면 안 되는 구조'가 먼저 작동한 것이 신뢰 훼손의 한 원인이었다고 생각합니다.
셋째, 감정을 증폭하는 미디어 환경과 정치화입니다. 확률이 낮은 사건은 서사가 강할수록 크게 느껴집니다. 알고리즘은 분노와 두려움에 더 큰 가중치를 둡니다. 자극적이고 왜곡된 기사는 단기간에 수십만의 조회수를 기록하지만, 전문가의 과학적 반박은 대중에게 도달하지 못합니다. 또 유튜브 쇼츠, 텔레그램 등의 알고리즘은 백신 회의주의 성향의 콘텐츠를 지속적으로 노출시켜 확증 편향을 강화하고, 저와 같은 전문가들과 공중보건 당국의 대응 속도를 무력화합니다.이 글만해도 참 쓰는데 오랜 시간이 걸렸습니다. 죄송합니다.
- 그 결과 대부분이 안전하게 접종을 마쳤다는 평범한 진실은 잘 보이지 않고, 개별 사례만 반복 노출됩니다. 여기에 과학과 정책의 영역에 머물러야 할 백신이 정치화되면서, 집권 세력에 대한 지지 여부가 백신 수용성에 영향을 미치는 현상이 고착화되었습니다.
- 이 세 가지는 백신 그 자체의 문제라기보다는, 우리가 위험을 해석하고 대응하는 방식의 문제입니다. 그리고 이것이 해결되지 않으면 다음 팬데믹에서 우리는 똑같은 실수를 반복하게 됩니다.
6. 지금 전세계에서 이상한 일이 일어나고 있습니다.
- 올해 미국은 25년 만에 가장 큰 규모의 홍역 유행을 겪고 있습니다. 2년 사이 수천 건이 넘는 확진자가 발생했고, 어린이 사망도 보고되었습니다. 확진자의 약 93%가 미접종자 혹은 접종력 확인되지 않습니다. (US CDC, 2026.4). 이제 미국은 홍역 퇴치국 지위가 흔들리고 있습니다.
- 우리나라에서도 백신 접종률은 조용히, 그러나 분명히 떨어지고 있습니다. 일부 정치적·이념적 언어로 백신 정책과 연구자 개인을 공격하는 흐름도 있습니다. 과학적 토론은 언제나 환영하지만, 근거 없이 공포를 증폭하는 것은 결국 가장 약한 사람들(아직 면역이 없는 영유아, 면역저하자, 고령자)을 해칩니다. 백신 불신이 단순히 개인의 선택 문제를 넘어, 사회적 연대의 도구인 집단면역의 붕괴를 초래할 수 있다는 점을 우리 모두 기억해야 합니다.
- 홍역은 기초재생산수(R₀)가 12~18에 달하는 인류가 아는 가장 전염력이 강한 바이러스 중 하나입니다. 집단면역 95% 선이 무너지면 유행은 반드시 돌아옵니다. 과학적 근거가 정치적 수사와 언론의 상업성에 의해 왜곡되는 현 상황은, 홍역 등 퇴치 수준에 이르렀던 감염병이 다시 유행하고 수 많은 아이들이 희생되었던 과거가 반복될 수 있을 지경에 이르렀습니다.
- 저는 백신이 만능이라고 말하지 않습니다. 드문 이상반응이 존재하지 않는다고도 말하지 않습니다. 모든 의학적 개입은 당연히 편익과 위험을 함께 갖습니다.
- 다만 지금까지의 가장 좋은 증거는 이렇게 말합니다.
'편익이 위험을 크게, 분명히 앞섭니다. 그리고 백신의 위험을 말하지 않기 위해서가 아니라, 말할 수 있을 만큼 많은 데이터를 우리가 가지고 있기 때문에 우리는 안심하고 이 이야기를 할 수 있습니다.'
- 불안한 마음에 이 글을 읽으셨다면, 그 마음이 틀린 것이 아니라 자연스러운 것이라는 말씀부터 드리고 싶습니다. 다만 불안이 결정으로 이어지지 않게 이렇게 한 번쯤 숫자와 연구를 함께 봐주시면 좋겠습니다.
- 저도 계속 연구하고, 데이터가 바뀌면 생각도 바꿀 것입니다. 그것이 과학의 태도이고, 제가 할 수 있는 최선의 백신에 대한 변호입니다.
Associate Professor, MD, PhD
Department of Preventive Medicine
Korea University College of Medicine
대한예방의학회/능인고등학교/고려대학교 의과대학
Basic Principles the Author Failed to Respect
Final integrated critique of the text’s statistical, inferential, and rhetorical weaknesses
The central problem with this text is not that it cites data, acknowledges rare adverse events, or argues that vaccines delivered substantial public-health benefits. The problem is that it repeatedly draws conclusions that go beyond what its own data and methods can legitimately support. It presents itself as a calm, data-driven clarification, but its actual structure is closer to institutional advocacy than to balanced analytical evaluation.
1. It does not distinguish descriptive data from causal inference
One of the text’s core moves is to take descriptive population-level trends—monthly mortality curves, age-stratified mortality patterns, aggregate cancer incidence—and use them to imply causal conclusions. That is the first major methodological breach. Descriptive trends can show that no large, obvious population-level rupture is visible in a given period. They cannot, by themselves, establish that vaccination did not contribute to harm, nor can they cleanly separate the effects of infection, vaccination, healthcare capacity, behavioral changes, or shifting access to care. The author repeatedly moves from “this pattern was not visibly disrupted” to “therefore the vaccine was not the cause,” which is a stronger claim than the design allows.
2. It confuses absence of a gross signal with absence of an effect
This is one of the most important inferential errors in the text. The author’s logic repeatedly relies on the idea that if there had been meaningful vaccine-related harm, one would have seen a strong upward deviation in aggregate mortality or cancer incidence during the mass-vaccination period. That is not methodologically sound. A real adverse effect may be rare, temporally concentrated, restricted to particular age or sex groups, diluted in all-cause outcomes, or partially offset by reductions in severe infection. In those cases, the signal may not appear as a dramatic shift in coarse population-level curves. A missing crude signal is not proof of no contribution. At most, it weakens the case for a large, obvious population-wide effect.
3. It treats heterogeneous exposures as though they were a single uniform intervention
The text repeatedly refers to “the vaccine” as if 2021 involved one homogeneous exposure. It did not. The vaccination period included different platforms, different products, different age-group distributions, different dosing intervals, and later booster-related shifts. That heterogeneity matters. Once exposures are heterogeneous, any claim drawn from aggregate post-vaccination outcomes becomes much weaker unless product-level, age-level, dose-level, and time-since-dose distinctions are preserved. The text collapses that complexity and then uses the simplified category to make broad claims about safety and downstream outcomes. That is structurally weak.
4. It does not sufficiently account for competing explanations
The text repeatedly interprets low excess mortality in 2021 as if it were strong evidence in favor of vaccine safety. But low excess mortality in that period could also reflect multiple other factors: lower severe viral burden before later waves, non-pharmaceutical interventions, reduced circulation of other respiratory pathogens, preserved hospital capacity, changes in healthcare utilization, and protection of high-risk groups through a combination of measures. A competent analysis does not merely mention one favored explanation and move on. It must show that competing explanations were controlled for, or at least explicitly weighed. Here, the competition between explanations is not treated symmetrically.
5. It relies on projections and counterfactuals without making the modeling basis transparent
The text repeatedly states that observed mortality or cancer incidence did not differ from projected or counterfactual expectations. That is a serious claim, but the underlying modeling structure is not adequately exposed in the prose. If one says an observed series stayed within a 99% prediction interval, the obvious questions are: What baseline period was used? Which model generated the prediction? How were age structure, secular trends, seasonal effects, delayed diagnoses, coding shifts, and pandemic-era disruptions handled? How wide were the intervals, and how sensitive were the conclusions to alternative specifications? Without those details, the statement sounds rigorous while remaining only partially auditable. The conclusion is strong, but the modeling transparency is insufficiently matched to that strength.
6. It overstates what age-stratified analysis can prove
The text presents age-specific mortality and incidence patterns as if stratification itself resolved the causal ambiguity. It does not. Splitting the data by age may improve descriptive resolution, but it still does not isolate infection effects from vaccine effects, healthcare disruption, baseline disease burden, deferred treatment, or administrative changes. Age stratification is not causal separation. The text treats it as if it were. That is another case in which the form of analysis is made to carry more inferential weight than it deserves.
7. It uses an overly closed causal frame: infection or vaccine
A recurrent structure in the piece is this: mortality did not rise sharply during early vaccination; mortality rose later during Delta or Omicron; therefore the rise belongs to infection, not vaccination. That frame is too binary. In reality, infection can be the dominant driver while small vaccine-related contributions still exist in subgroups. Healthcare-system strain and indirect harms can coexist with both. Different products, ages, and periods can carry different risk-benefit balances. The text repeatedly turns a complex causal field into a clean either-or narrative. That is analytically convenient, but methodologically reductive.
8. In the cancer section, it extends short-term aggregate stability too far
The cancer section contains one of the most overextended argumentative moves in the document. The strongest defensible claim from the described data is that, at the population level and within the observed short time window, no large deviation from prior cancer-incidence trends was detected after mass vaccination. That is materially different from implying that vaccination did not contribute to cancer risk. Cancer is heterogeneous, often latency-dependent, affected by screening patterns, diagnosis delays, claims behavior, and coding practices. The text does acknowledge screening disruption in 2020 and rebound effects in 2021, but then still uses the post-2021 stability to support a broader reassuring conclusion than the timeframe and data structure can justify. It also aggregates highly heterogeneous cancer categories into a single rhetorical conclusion: “all 12 cancer types show the same conclusion.” That is too sweeping for a phenomenon with divergent biology and detection pathways.
9. It repeatedly turns non-significance into no change
Another recurring problem is the treatment of non-significant findings as though they established no effect or no shift. A statistically non-significant level or slope change means that the model did not detect a sufficiently clear deviation under the chosen assumptions and available data. It does not mean the true change was zero. It does not mean subtle, subgroup-specific, or longer-latency shifts are excluded. This is one of the most common bio-statistical misreadings, and the text leans on it too often.
10. It compares collective benefits and individual harms on unequal terms
In the adverse-event section, the text argues that collective benefits greatly outweigh rare severe risks. That proposition may well be true in important populations, especially older adults. But the argument is built by juxtaposing different analytical layers: massive modeled global death-prevention estimates, Korean elderly protection estimates, and rare individual-level adverse events such as myocarditis or TTS. Those numbers are not illegitimate, but they do not sit on the same interpretive plane. Population-level lives-saved estimates and individual-level harm probabilities require careful framing, subgroup specification, and temporal qualification. Instead, the text uses them in a single directional flow toward reassurance. This makes the overall structure rhetorically effective, but analytically flatter than it should be.
11. It uses model-based global estimates too definitively
The reference to nearly 20 million global deaths prevented in the first year of vaccination is a model-based counterfactual estimate, not a directly observed tally. Such estimates can be important and informative, but they depend on assumptions. The text presents them with very little emphasis on uncertainty, scenario sensitivity, or the fact that those estimates do not automatically transfer to individual Korean risk judgments. Once again, the document takes something plausible and substantively meaningful, then presents it with more closure than its modeling basis warrants.
12. It overgeneralizes from elderly benefit to the whole population
High protection against severe disease and death in older adults is a powerful public-health point. But it does not automatically settle the risk-benefit balance for younger groups, different sexes, different vaccine products, or booster-era conditions. The text moves too quickly from “the most vulnerable were strongly protected” to a more generalized moral and scientific reassurance. That leap compresses heterogeneity into a single unified message.
13. It treats the existence of surveillance systems as though that resolved the interpretive problem
The text points to large-scale surveillance and reporting systems as evidence that the safety database is vast and therefore that the risks are known and discussable. That is partly fair. But the existence of many surveillance systems is not the same thing as complete causal clarity. Surveillance systems have underreporting, reporting bias, case-verification limits, temporal ambiguity, and varying sensitivity to rare or delayed events. Saying “we have a lot of data” is not equivalent to saying “the interpretation is settled.” The text slides too easily from data volume to interpretive confidence.
14. It says it is transparent about risk, but structurally reabsorbs risk into defense
The text repeatedly states that rare but serious adverse events are real and should not be hidden. On the surface, that is a strength. But the paragraph structure consistently follows the same pattern: acknowledge a risk, immediately place it within a much larger benefit frame, then reinforce the size and legitimacy of the safety database. That is not outright concealment, but it is not neutral balancing either. The risk is admitted only to be rapidly subordinated within the overall defense architecture.
15. It psychologizes distrust more than it structurally analyzes it
In the section on why people became suspicious of vaccines, the text shifts away from science and toward human emotion, experience, media amplification, and politicization. Some of that is valid. But the overall result is to explain distrust primarily as a function of risk misinterpretation, algorithmic emotional amplification, and political distortion. That framing risks absorbing rational skepticism, legitimate grievances, policy coercion, poor communication, weak compensation mechanisms, and institutional failures into a largely psychological narrative. It makes the public easier to diagnose than the system.
16. It softens institutional responsibility while emphasizing external distortions
The author does admit that compensation and recognition for adverse-event sufferers were insufficiently warm and that uncertainty was oversimplified. But the deeper structural responsibility of institutions is underdeveloped. Instead, the piece gives more explanatory weight to distorted media, politicization, and audience misperception. That asymmetry matters. The public-health system is treated as imperfect but fundamentally corrective, while the environment around it is treated as the main destabilizing force. That is a defensive rather than symmetrical allocation of responsibility.
17. It blurs the line between rational critique and manipulative fear
The text says scientific debate is welcome, yet repeatedly places skepticism in close proximity to fear amplification, distorted media narratives, and ideological attacks. That rhetorical proximity weakens the distinction between evidence-based criticism and irrational agitation. A stronger analytical text would separate those categories clearly. This one does not do so consistently.
18. It ends by shifting from COVID-vaccine debate to measles and herd immunity
This is one of the clearest rhetorical maneuvers in the document. The final section moves from the contested terrain of COVID-vaccine safety and risk-benefit interpretation into the much more settled public-health terrain of measles outbreaks, herd immunity thresholds, and vulnerable children. That move is persuasive, but it is also a change of battlefield. It allows the text to borrow the moral and epidemiological clarity of measles immunization in order to reinforce its broader warning about vaccine distrust. The linkage is not wholly illegitimate, but it is not direct proof of the earlier claims either. It is rhetorical reinforcement by adjacency.
19. It moralizes doubt by connecting it to social harm
The closing argument strongly suggests that distrust in vaccines is not just a personal cognitive issue but a social threat that can damage collective protection and harm the weakest. Again, this may have public-health logic in some contexts. But analytically, it also means that doubt is no longer treated simply as a question to be examined; it becomes a morally charged social risk. Once that happens, criticism is harder to treat as legitimate scrutiny and easier to frame as dangerous destabilization. That is a shift from analysis toward normative persuasion.
20. It declares openness to future evidence, but the overall structure is already closed
The author ends by saying that if the data change, his view will change. That is the correct scientific posture in principle. But the overall architecture of the document is not open-ended. It is already arranged toward a destination: reassurance, defense, and containment of distrust. The statement of openness does not erase the fact that the preceding analysis has been built in a strongly conclusion-directed way.
When Defensive Inference Becomes a Systemic Risk
Why conclusion-first evidence culture in the Korean pharmaceutical sector would materially elevate stakeholder and due diligence risk
If the inferential logic displayed in this text is not an isolated author-level failure but instead reflects a broader pattern within the Korean pharmaceutical and regulatory ecosystem, then the problem is no longer merely academic. It becomes a systemic risk. The core danger is straightforward: once evidence is used primarily to defend a preferred institutional conclusion rather than to test competing explanations symmetrically, biostatistics ceases to function as a falsification tool and becomes a mechanism of narrative stabilization. In that environment, uncertainty is managed rather than examined, model outputs are treated as closure rather than conditional inference, and weak inferential discipline can be mistaken for scientific confidence.
For stakeholders, this creates a dangerous distortion layer between underlying reality and reported interpretation. Regulators may believe they are protecting public trust while actually weakening evidentiary integrity. Academic investigators may appear rigorous while embedding conclusion-first logic into study framing, endpoint interpretation, and public communication. Companies may internalize the same culture and produce safety, efficacy, or post-marketing narratives that look statistically respectable yet remain structurally biased toward institutional preservation. The result is not simply a communication problem. It is an evidentiary governance problem.
For investors, this has direct due diligence implications. If a conclusion-first statistical culture is common, then published analyses, internal safety narratives, real-world evidence packages, post-marketing signal assessments, and regulatory briefing materials cannot be read at face value. The key question is no longer whether a dataset exists, but whether the inferential architecture surrounding that dataset is trustworthy. Investors should therefore examine whether the company and its external experts clearly distinguish descriptive trends from causal claims, disclose model assumptions transparently, test competing hypotheses symmetrically, separate non-significance from absence of effect, and show genuine sensitivity analysis rather than rhetorical certainty. Where those disciplines are weak, the risk is not only scientific error but valuation error, regulatory surprise, reputational shock, and delayed recognition of safety or execution failures.
This is precisely where a more disciplined Bayesian-regulatory future becomes relevant. A system built on continuous updating, explicit priors, auditable assumptions, and sensitivity to incoming evidence is inherently hostile to static conclusion-first storytelling. But that only helps if methodological integrity is real. If the same defensive logic enters the model itself, bias does not disappear; it becomes mathematically polished. That is why this issue should matter to every stakeholder in the Korean biopharmaceutical chain, and especially to investors. In a sector where trust, regulation, and capital formation all depend on evidentiary credibility, weak inferential culture is not a minor academic flaw. It is a material risk factor.